When Diseases Travel Together: Insights from Endometriosis Patients
Khan et al. analyzed one of the largest collections of health records from endometriosis to date, with patients drawn from several University of California databases, including a separate database from the University of California, San Francisco. In doing so, they found several comorbidities that occurred more frequently in endometriosis patients than in matched healthy controls. This was supported not only by prior literature but also by an orthogonal approach that identified patient subgroups characterized by many of the same comorbidities.
Written by Ethan Hung, Schematic by Lexi Bean
What is this study about?
Endometriosis (EM) is a condition not often spoken about, perhaps one you’ve never heard of. But for how disruptive EM’s symptoms can be in daily life, EM is a challenging condition to tackle at several levels.
For one, EM only affects women and others assigned female at birth. But because EM disproportionately affects lower socioeconomic populations, this can add an additional layer of complexity. Given EM’s proximity to other forms of chronic pain, EM patients face a similar stigma that can make getting adequate treatment more difficult. Once a patient visits a clinician, EM diagnosis remains a challenge. Many of the first symptoms are typically common ones, like bleeding and abdominal pain, that are triggered by many other conditions. This means EM is often a diagnosis of exclusion, but once EM is suspected, a surgical biopsy is still necessary for a definitive diagnosis. As you might guess, these factors may cause individuals to delay or avoid medical care altogether, making EM even harder to study on a larger scale.
Once EM is diagnosed, that’s just the first step. Scientists know that EM occurs when the tissue lining the female reproductive system grows in places where it's not supposed to (but not in a cancerous, uncontrollable way). But there’s still a lot we don’t know at a fundamental level, and this limits the options for treating or preventing EM. For severe cases, the most effective treatment is hysterectomy, an invasive surgical procedure that comes at the cost of infertility. But for the majority of patients, living with EM is a trial-and-error process aimed at managing their symptoms. To tackle this disease, we need to learn a lot more. That brings us to why the authors of this paper, led by Umair Khan and the Sirota lab at UCSF, needed a bird’s-eye view to look at the landscape of EM.
How was it conducted?
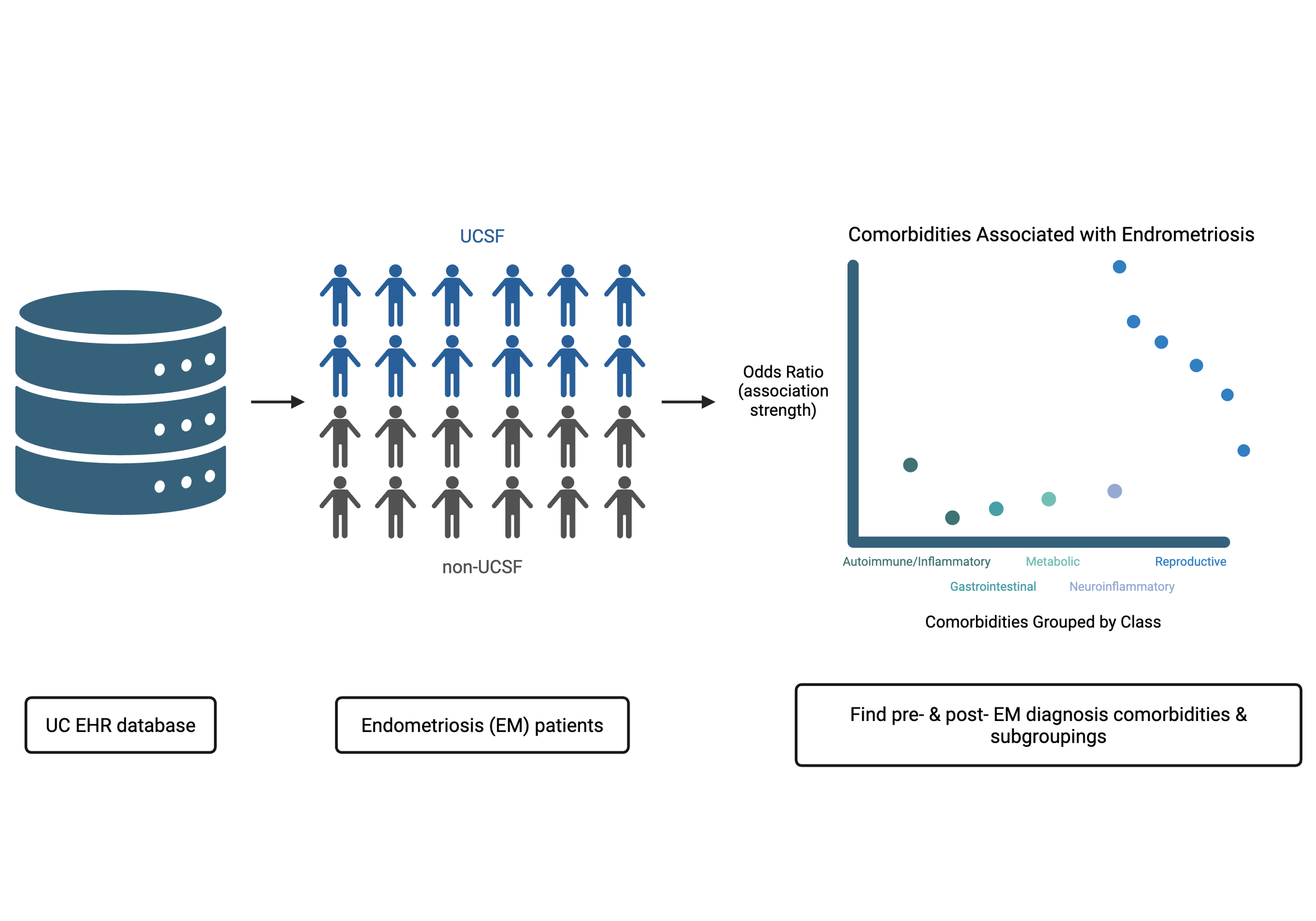
To better understand how EM develops and what biological processes could be related, the authors started by examining patterns in patients’ medical histories. This is important because while prior studies have tried to connect EM to other conditions, or comorbidities*, the broader picture of which diseases are most associated with EM is not as well characterized. To get this overview, they looked at EM patients’ electronic health records (EHRs).
After collecting diagnoses recorded during medical visits for these patients, the authors wanted to determine if any medical conditions were more common in EM versus healthy patients. They do this by asking: how many EM patients have Condition X (AEM) versus not (BEM)? Taking a ratio of the two (AEM/BEM) and the same for matched controls (ACTL/BCTL), we can find the odds ratio of a Condition X for EM patients (AEM/BEM ÷ ACTL/BCTL)†. Conditions with the highest odds ratio are those that most frequently co-occur in EM patients. If we assume some shared biology connects EM and a comorbidity, those with the highest odds ratios are the most interesting candidates to further pursue.
Something worth noting: In this study, the authors took advantage of the combined resources of the statewide University of California (UC) medical centers to get the deidentified records of over 40,000 EM patients. Not only was this one of the first studies on such a large scale, but the patients were nearly evenly split between the UCSF-specific patients and those from other UC campuses. By validating their analysis on two separate databases, the authors found that their results were well-aligned, allowing us to place more confidence in the findings of the authors’ results.
What did they learn?
Over 600 comorbidities were identified, but the most strongly implicated conditions had been previously associated with endometriosis, like: uterine adenomyosis (similar to EM but occurring inside the uterus), pelvic peritoneal adhesions (pain caused by scar tissue in the pelvic region), EM-associated infertility, and autoimmune conditions. However, some conditions identified were less commonly associated with EM; for example hyperlipidemia, migraines, asthma, vitamin D deficiency, and gastrointestinal conditions like heartburn and Crohn’s disease. While previous studies have suggested a potential link between EM and these conditions, these observations in EM patients have never been explicitly identified in health record data nor causally linked with EM. Moreover, unbiased clustering of this EHR data also identified subgroups of patients that shared many of these conditions. As such, they remain useful hypotheses for future study.
When focusing solely on comorbidities identified before EM diagnosis, several genitourinary conditions stood out, such as dysmenorrhea, ovarian cysts, and pelvic pain. Also, high levels of cancer antigen 125, a common biomarker for ovarian cancer risk and previously implicated in EM, were notably identified as well. Interestingly, hyperlipidemia was negatively associated in this pre-EM analysis -- the authors note that previous studies have suggested statins (which patients with hyperlipidemia would likely be taking) as a potential EM treatment.
There’s a lot here for scientists to dig further at, but there’s also limitations to keep in mind. Like most others, this study was limited by sample biases, both known and unknown. For example, patients with well-represented health records are likely to have better access to medical care and higher socioeconomic status. Conversely, this means that patients from less affluent backgrounds are underrepresented in EHR data. Patients might also have gaps in their records (maybe they moved away from California!) that aren’t equally represented nor easy to control for. Such challenges can lead to unpredictable biases in demographic representation. Finally, it’s important to note that these observations only identify correlation or co-occurrence rather than causation. That means this analysis can’t say whether (1) A affects B, (2) vice versa, or (3) if A & B are unrelated while a separate C affects both. For example: regarding adenomyosis (the top EM comorbidity by odds ratio), the authors acknowledge that “adenomyosis and endometriosis are sometimes conflated” because of how the EHR is structured. In this case, the shared biology is well-understood and accepted. But in other cases, the line can be more blurry.
Ultimately, this study was exploratory in nature. While it was never designed to have the final say on whether any specific condition is causally related to EM, it has opened the field to new ideas. This study in particular provides additional evidence for various hypotheses, such as implicating conditions with less experimental support like hyperlipidemia, migraines, and vitamin D deficiency, as well as suggesting that statin treatment for hyperlipidemia may lower EM risk. As such, studies like these are important for getting a bigger picture of where we are in the fight against EM and hopefully, where we’ll be going.
A link to the full publication can be found here: https://www.sciencedirect.com/science/article/pii/S2666379125003180?via%3Dihub
Footnotes:
* Technically, the word “comorbidity” is usually defined by co-occurrence (AKA at the same time). But because disease processes can be a slow, considering conditions that occur before/after EM diagnosis is still useful. That’s why you can interpret the word as “a condition that’s likely related to another”.
† They actually do this several times by splitting the EM patients (and matched controls) into 30 groups to get 30 odds ratios. This sample distribution of odds ratios helps the authors identify comorbidities where the odds ratio is relevant -- but likely not just by chance (Bonferroni-adjusted p-value < 0.05).