Repairing the Brake Pedals of the Immune System with CRISPR
Written by Scarlett Yang, Schematic by Lexi Bean & Scarlett Yang
Our immune system is supposed to protect us from various threats, but what happens if it turns against us and starts attacking the body?
This is the problem behind autoimmune diseases, where the immune system gets confused about “self” and “non-self.” Sometimes, such confusion starts in the gene. A small mutation (an error in the DNA sequence) can disrupt how the cells of the immune system develop and function. These genetic conditions are called inborn errors of immunity. Some errors weaken the immune system, making the patient more vulnerable to infections, while others can make it overly aggressive, attacking the body itself.
In one patient with a rare genetic immune disorder named IL2RA deficiency, her immune system became overactive, affecting various parts of her body. It attacked her red blood cells, which carried oxygen in her blood, platelets, which helped stop bleeding, as well as other immune cells. She also experienced skin inflammation, mouth ulcers, and repeated ear infections. Taken together, these seemingly unrelated symptoms were the clues that pointed to a broken immune system.
Researchers from UCSF and collaborating institutions, led by Dr. Brian R. Shy and Dr. Jonathan H. Esensten, aimed to address the problem and have developed a potential therapy. In their recent paper published in Molecular Therapy in 2025, they applied the gene-editing tool CRISPR-Cas9 to correct the disease-causing mutation, correcting IL2RA deficiency and restoring normal immune function.
Brakes of the immune system: regulatory T cells
T cells are one type of immune cell that protects the body from infection and disease. Some T cells recognize pathogenic invaders and abnormal cells that are infected or cancerous, killing them directly; others can instruct, help, and coordinate other immune cells. Normally, T cells focus only on the “bad guys,” but they can sometimes make mistakes. Some T cells may recognize the body’s normal cells as threats and attack them, resulting in autoimmune diseases.
To prevent this, the immune system has internal “brakes” that help suppress aggressive T cells. One of these brakes is a specific type of T cell, termed a regulatory T cell, or Treg. As their name suggests, Tregs regulate immune activity. They inhibit the activation and amplification of self-reactive T cells, reducing the risk of developing autoimmune disease.
But Tregs also need signals to survive and function. One crucial signaling molecule is IL-2 (interleukin-2), which controls the development, survival, and function of Tregs. To receive the signals and instructions from IL-2, Tregs use the IL-2 receptor (IL-2R) on the cell surface to bind IL-2. One component, IL2RA, helps increase the affinity of IL-2R and better capture IL-2.
However, if the gene encoding IL2RA has a mistake (mutations), IL2RA will become deficient. Tregs that lack IL2RAs can become partially “blind” to IL-2, failing to receive its signals and eventually losing their ability to suppress overaggressive immune cells. Self-attacking T cells can now escape from surveillance and damage normal cells in the body. This is when “autoimmunity,” or immunity against self, occurs (Fig. 1).
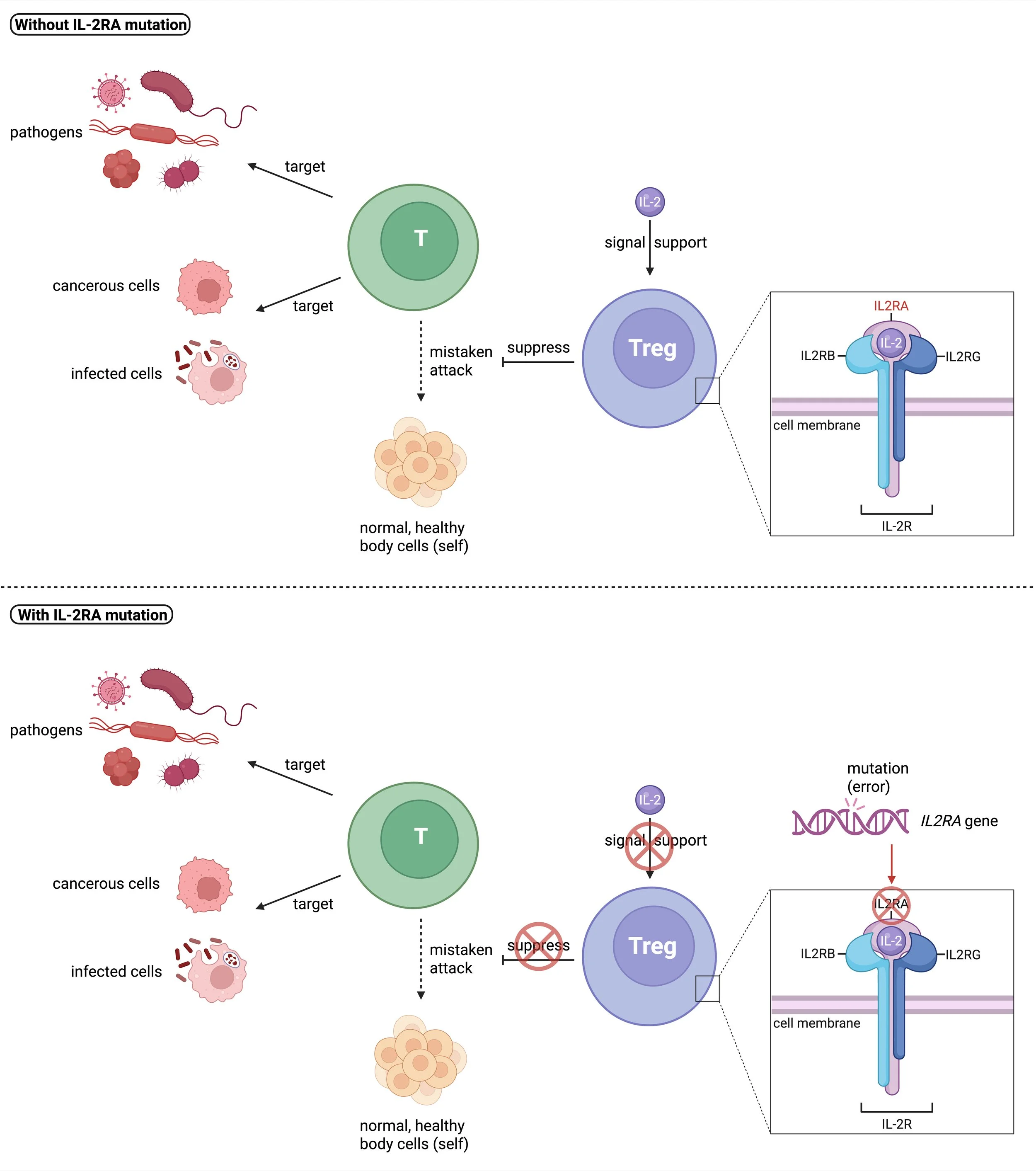
Fig. 1: IL-2RA mutations disrupt Treg function. Top panel: Tregs receive signals from IL-2 and suppress T cell immune response toward the self. Bottom panel: effects of IL-2RA mutations.
How does the therapy work?
Targeting this mutation, the researchers have developed a potential novel therapy to restore Treg function. The goal is simple and precise: take the patient’s cells out, fix the mistakes outside the patient’s body, and then prepare the fixed cells to be put back into the patient.
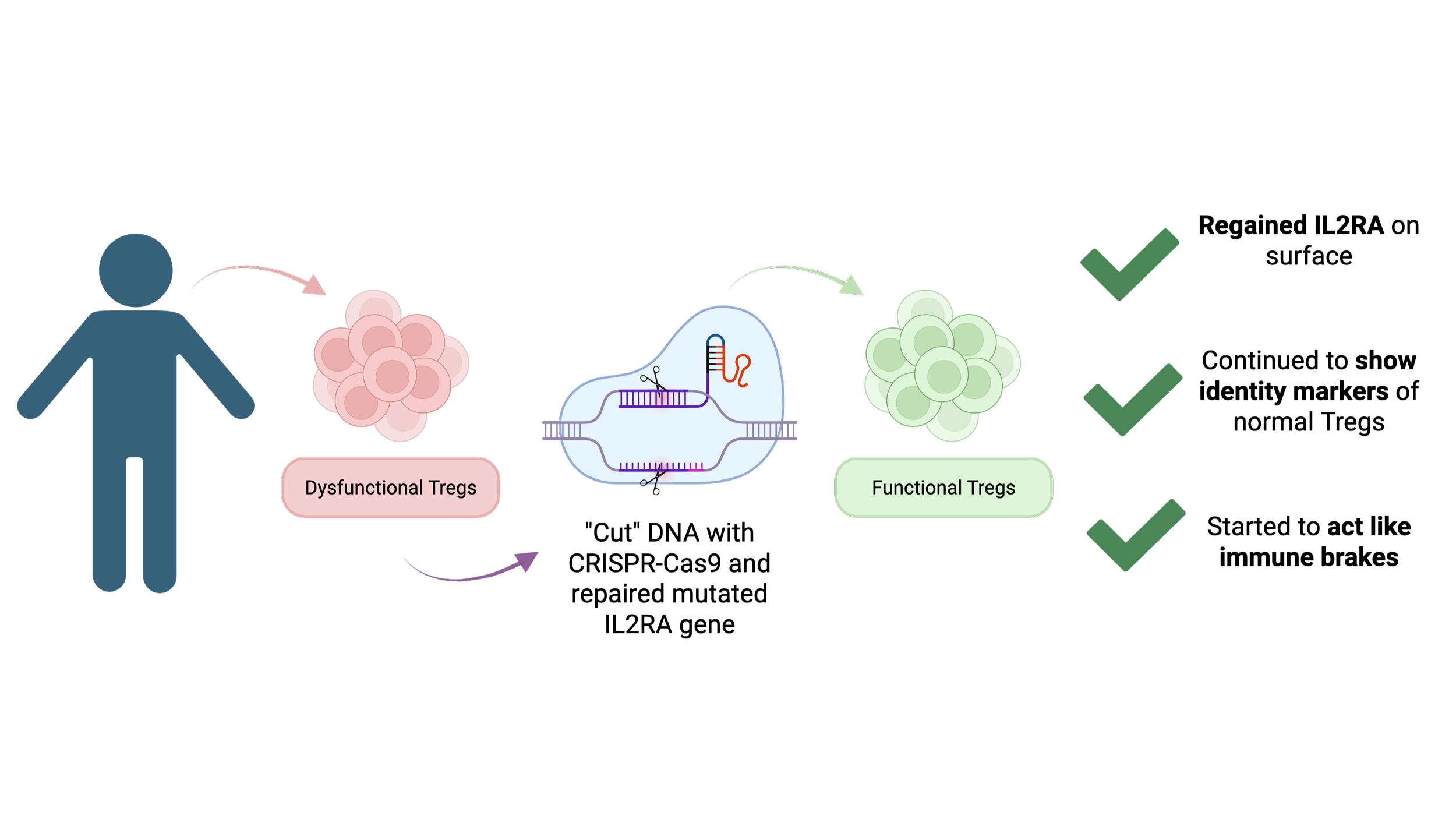
The researchers first collected blood cells from the patient who had an IL2RA mutation. Among the blood cells, they selected Tregs in particular. So now, they can do some magic to the Tregs with CRISPR-Cas9. CRISPR-Cas9 is often described as “molecular scissors” that can be guided to cut DNA at a specific location. In this study, the researchers used this pair of scissors to cut the mutated IL2RA gene and provided a template to rewrite the mutated part correctly. Afterwards, the researchers grew more of these repaired Tregs in cell culture and purified those that could express IL2RA into a final product (Fig. 2).
Of course, the researchers still needed to test whether this method and the repaired Tregs actually worked. They asked three main questions:
Was the IL2RA gene accurately corrected?
Did the cells look like true Tregs?
Did the cells function like Tregs?
The answers were encouraging. First, the repaired Tregs regained IL2RA on their surface, still possessed essential identity markers of normal Tregs, and were able to suppress other T cells in lab tests. In other words, the corrected Tregs not only looked repaired, but also started acting like immune brakes again!
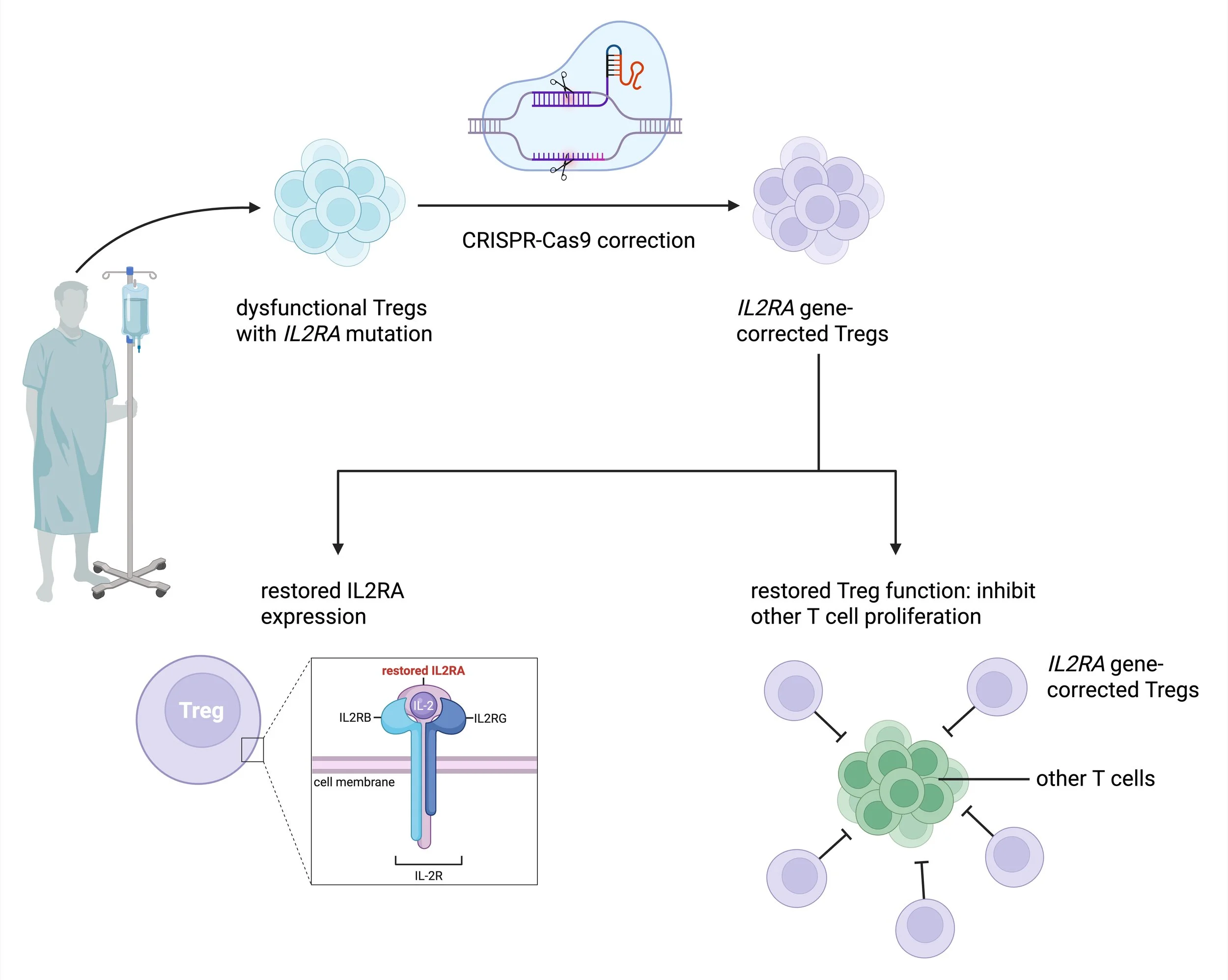
Fig. 2: Workflow of gene-corrected regulatory T cell therapy. CRISPR-Cas9 correction restores IL2RA expression and normal Treg function.
Why does it matter?
Current treatment options for IL2RA deficiency and subsequent autoimmunity are still limited. They include drugs that suppress the entire immune system throughout the patients’ lifetime. While this immunosuppression can reduce the immune system’s attacks against the self, it does not cure the disease fundamentally and weakens the patients’ immune system. So now, the patient’s immunity is no longer too robust but too weak. Thus, the patients become more vulnerable to various infections.
Another option is to transplant normal blood-forming stem cells from another individual into the patient’s bone marrow to rebuild the patient’s immune system. But this is tricky as well because a transplant carries huge risks, like rejection and even death. For both patients and doctors, there is no easy answer to choose between long-term immunosuppression and risky transplantation.
This is why the new design of Treg-based cell therapy is exciting. It carries a huge potential to avoid the disadvantages of the two treatments above. Unlike the immunosuppressive drugs, this targeted strategy corrects only dysfunctional Tregs, the natural brakes of the immune system, but does not affect the patient’s normal ability to fight infections. Meanwhile, unlike transplants, this new Treg correction uses the patient’s own cells rather than introducing cells from the donor. Since the corrected cells come from the patient themself, the strategy greatly reduces risks related to rejection.
Moreover, the new treatment strategy is meaningful not only to patients with IL2RA deficiency but also to treating rare genetic immune disorders. Many of these diseases are caused by certain mutations that break a step in the immune response. This study shows one possible model to fix the issue: collect the patient’s own cells, correct the mutation, and return the repaired cells to the patient. As CRISPR-Cas9 has been widely used as a research tool, this study exemplifies how the clinical world can harness the power of precision gene editing, enabling more personalized medicine.
However, this therapy is still at an early stage. The researchers have shown that dysfunctional Tregs can be corrected in the lab, but the therapy has not been proven effective inside the patient’s body. Concerns and questions remain: How many corrected cells need to be infused? How long will the effect last? Despite the uncertainties, this work offers a promising vision for a third option to treat inherited immune disorders.
References:
Image Reference:
Fig. 1: Created with Biorender: https://app.biorender.com/illustrations/6a0ce5d5c33212398911e7e9?slideId=72e7455c-a68a-4704-8610-443e5b44fa56
Fig. 2: Created with Biorender (adapted from the Ha et al. paper): https://app.biorender.com/illustrations/6a0ce5d5c33212398911e7e9?slideId=72e7455c-a68a-4704-8610-443e5b44fa56